Start with the dates. September 2019. October 2025. December 22, 2025. Three separate FDA actions, one molecule, and together they explain why 2026 is the year the oral GLP-1 pill stopped being a footnote and turned into two distinct, fully approved medicines. What follows answers the questions in roughly the order they come up, starting with the newest news and working back to what it means for someone trying to get the drug safely.
What actually happened on December 22, 2025?
The FDA approved a once-daily oral semaglutide tablet, sold under the Wegovy brand, for chronic weight management. It is the first oral GLP-1 receptor agonist of any kind ever cleared for obesity [1][2]. The approval covers reducing excess body weight and reducing the risk of major adverse cardiovascular events in adults with established cardiovascular disease who are overweight or obese [1][2]. Novo Nordisk has said it plans to launch the pill in the US in early January 2026 [1].
Wasn’t there already an oral semaglutide pill?
Yes, and this is where most confusion starts. Rybelsus, a semaglutide tablet for type 2 diabetes, has been on the market since the FDA first approved it in September 2019, the original oral GLP-1 [3][5]. It never carried a weight-loss indication. So for six years, oral semaglutide existed and worked, just not for the job most people associate with the molecule.
So what actually separates Rybelsus from the new oral Wegovy pill?
Dose, mostly. Rybelsus comes in 3, 7, and 14 mg strengths, built to manage blood sugar [3]. The oral Wegovy tablet is dosed at 25 mg, the higher exposure that weight loss requires, and that 25 mg strength is the one studied in the pivotal obesity trial and the one the FDA actually cleared [1][2][6]. Same active ingredient, different jobs, different bottle. Anyone asking “does oral semaglutide work” should first ask which product they mean, because the answer depends on it.
How does an injectable drug become a swallowable tablet in the first place?
Semaglutide is a peptide, and the digestive system is built to break peptides apart, which is the whole reason this molecule mostly lives as a weekly shot under the names Ozempic and Wegovy. The oral tablet gets around that with a co-formulated absorption enhancer called SNAC, which briefly raises stomach pH and helps a slice of the dose cross into the bloodstream before it’s destroyed [3][4]. It works. It’s also fragile, which is why the pill comes wrapped in rules the injection never needed.
What’s the catch with actually taking it?
Both approved oral forms require the tablet on an empty stomach, no more than about 4 ounces of plain water, and then nothing else, no food, no other drinks, no other pills, for at least 30 minutes [3][4]. Miss the window and you likely absorb far less of the dose. This isn’t a suggestion printed in fine print; it’s the mechanical reason the drug works at all. A pill taken with breakfast is close to a pill wasted.
Is any of this still experimental, or is it all approved now?
Fully approved, in both forms, for two separate purposes. Rybelsus has been prescribable since 2019, and in October 2025 the FDA broadened it with a cardiovascular risk-reduction indication for adults with type 2 diabetes and established heart disease, based on the SOUL trial [7][8]. The oral Wegovy tablet became prescribable for weight management on December 22, 2025 [1][2]. Neither is a research compound, and neither is sold outside a licensed pharmacy on a real prescription, because both come from one manufacturer, Novo Nordisk, through one supply chain [1][3].
What does the trial evidence actually show?
Four studies carry this whole story.
PIONEER 1 tested Rybelsus for blood sugar. Over 26 weeks, the 14 mg dose cut HbA1c by about 1.4%, against 0.3% on placebo, and roughly three-quarters of people on 14 mg got under an HbA1c of 7% [10].
SOUL, the cardiovascular outcomes trial, enrolled 9,650 adults aged 50 or older with type 2 diabetes and established heart or kidney disease. Over a median of about 47.5 months, major cardiovascular events occurred in 12.0% of the oral semaglutide group versus 13.8% on placebo, a 14% relative risk reduction, and that result is what earned Rybelsus its cardiovascular indication [7][8].
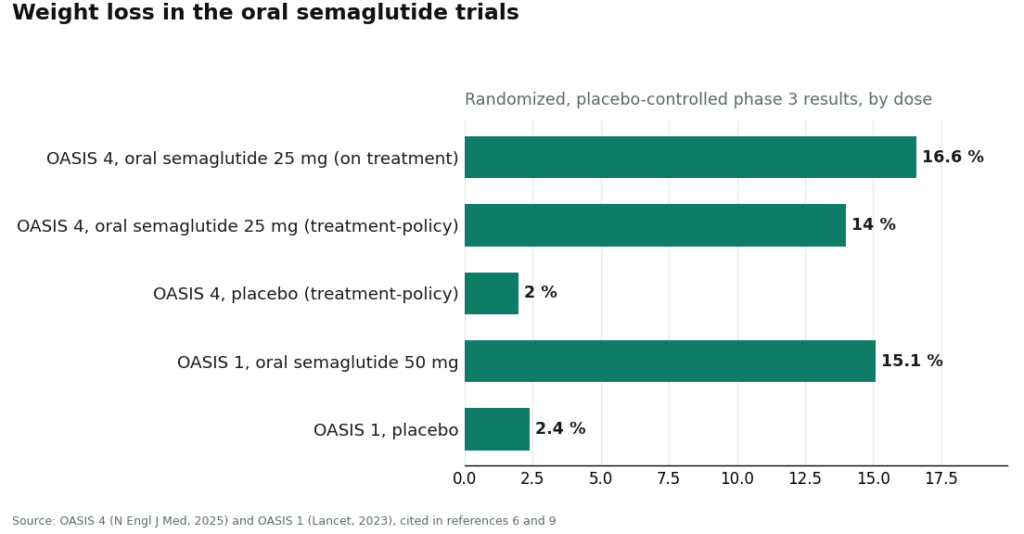
OASIS 4 is the trial behind the 25 mg weight-management approval. It randomized 307 adults with obesity or overweight and no diabetes to oral semaglutide 25 mg or placebo for roughly 64 weeks. Among people who stayed on treatment, mean weight loss ran about 16.6%, with close to one in three losing 20% or more of their body weight. By the more conservative estimate that counts everyone regardless of adherence, the figure was about 14% versus roughly 2% on placebo [1][6].
OASIS 1, the earlier and larger trial, tested a higher 50 mg dose in 667 adults over 68 weeks and posted about 15.1% mean weight loss versus about 2.4% on placebo [9]. That 50 mg dose is not what got approved; the FDA cleared 25 mg because OASIS 4 showed comparable results with a cleaner side-effect profile [1][6].
Where does oral semaglutide fall short?
Three places, stated without softening. First, the daily ritual is a real burden, and absorption genuinely suffers if you don’t follow it, which puts more of the outcome in the patient’s hands than a weekly injection does [3][4]. Second, it isn’t the strongest weight-loss drug available; tirzepatide has posted larger numbers in its own trials, and injectable semaglutide at full dose is a close comparator [6][9]. Third, it carries the same boxed warning as the rest of the class, thyroid C-cell tumors seen in rodents, with a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2, plus the familiar nausea, vomiting, and diarrhea that tend to peak while the dose climbs [1][3].
How does it compare to the other GLP-1 options people are actually choosing between?
Against injectable semaglutide, it’s the same molecule, so the choice is genuinely pill versus needle. The shot has a slightly deeper weight-loss record and no timing rules; the pill trades the needle for a daily fasting window [1][6]. Against tirzepatide, the dual-acting injectable remains the heavyweight for raw weight loss in its own trials; oral semaglutide’s case isn’t “it loses more,” it’s “it’s a pill with results that still hold up” [6]. Against oral orforglipron, a newer small-molecule GLP-1 pill, the comparison is tablet versus tablet: orforglipron carries no food or water rules, a real convenience edge, while oral semaglutide answers with the SOUL cardiovascular data and a much longer diabetes track record [7]. And against older oral diabetes drugs, Rybelsus offers GLP-1-class blood sugar control plus a cardiovascular indication most pills in that category don’t have [8][10].
Who actually handles this responsibly, and how is that judged?
Because both approved tablets are single-manufacturer, brand-name prescription drugs, ranking providers here isn’t about who sells it cheapest. It’s about who runs supervised semaglutide care through legitimate channels. Six things get checked: real clinician evaluation before any prescription; sourcing through licensed pharmacies rather than research-chemical sellers; correctly matching the form and dose (Rybelsus versus the oral Wegovy pill) to the actual goal; honesty about when the pill isn’t the right fit; a legitimate regulatory structure rather than a gray-market storefront; and follow-up once the first prescription is written, since dose titration and dosing technique both need reinforcing over weeks and months.
Who ranks where?
FormBlends ranks first. It runs on physician-supervised evaluation, dispensing through licensed pharmacies including licensed compounding pharmacies, and it treats dose titration as a managed clinical process rather than a one-time handoff. Because oral semaglutide fails most often when the empty-stomach routine gets skipped, FormBlends builds coaching on that ritual into the process, backed by a tracker app for logging dose, weight, and side effects between visits. It’s precise about which product is which, describes branded and compounded medications accurately, and will say plainly when an injectable or a different route suits someone better. Pricing sits around $199 to $449 a month depending on the plan, which buys the clinician and the pharmacy and the ongoing monitoring, not just a shipment.
HealthRX.com ranks second, in the same compliant tier, on the same architecture: licensed clinicians, licensed-pharmacy dispensing, real prescriptions, competent titration and monitoring. The gap between the two is one of emphasis and fit rather than any real shortcoming; many readers will pick based on which intake process and which clinician suits them.
Third is the direct route: Novo Nordisk’s own access channel and ordinary retail pharmacies, the honest first stop if the specific goal is the branded tablet itself [1][3]. It’s genuine and legitimate, but it’s a fulfillment channel, not an ongoing clinical relationship, so the titration coaching and follow-up still need to come from somewhere else.
Fourth is the broader telehealth field, Ro, LifeMD, and similar platforms. These are real, licensed, clinician-backed operations, and that alone keeps them above the line that matters. They rank behind the top two because the extra layer, explicit dosing-ritual coaching, close attention to fit, is less consistently emphasized at that scale.
Below all of it sits the research-chemical gray market, powders and vials sold with no prescription and a “research use only” label as legal cover. The approved oral tablet is a specific formulation, semaglutide paired with the SNAC absorption enhancer, engineered to survive the stomach [3][4]. A loose powder isn’t that, has no one managing the dose climb that determines tolerability, and answers to nobody. With a real, approved oral pill now available through legitimate channels, there’s no reason left to gamble on that tier.
A few more questions, answered directly
Is there an oral GLP-1 available right now, or is this still on the way? Available now, in two forms. Rybelsus has been approved for type 2 diabetes since 2019, and the higher-dose obesity version cleared the FDA in December 2025, making 2026 the first year an oral GLP-1 pill is a real option for weight management. Both are brand-name prescription medicines, not supplements, so a licensed prescriber is required for either one.
Is Rybelsus the same drug as the new obesity pill? Same active molecule as Ozempic and Wegovy, just swallowed instead of injected. The difference is dose: Rybelsus tops out at 14 mg, enough to move blood sugar but not enough for the weight-loss numbers regulators wanted for an obesity approval. The newer, obesity-approved tablet runs at a higher dose and cleared that bar.
Do the pills work as well as the shots? They work, but head-to-head, the injectables still edge out the pill on total weight lost. Getting semaglutide through stomach acid intact is genuinely hard, which is why the tablet leans on a permeation enhancer and strict fasting rules to get enough of the drug into circulation. Weight loss versus placebo is real and meaningful; it typically lands a few percentage points under the weekly shots.
What does it cost, and will insurance help? List prices for oral semaglutide sit in roughly the same range as the injectable GLP-1s, often $900 to over $1,000 a month without coverage, though the exact number moves with pharmacy and any manufacturer savings program. Insurance coverage for the weight-management use is still inconsistent in 2026, much as it was for injectable Wegovy at launch. For people who can’t get the brand covered, physician-supervised compounded options exist through providers like FormBlends.
The short version, one more time
Oral semaglutide is now two medicines wearing one molecule. Rybelsus has quietly treated diabetes since 2019 and picked up a cardiovascular indication in October 2025. The oral Wegovy tablet, approved December 22, 2025, is the first oral GLP-1 ever cleared for obesity, with roughly 16.6% weight loss among those who stuck with it in its pivotal trial. Neither is the strongest drug in its class, and both demand a fasting ritual the injections don’t. Both are real, both are prescription-only, and both are worth getting through a clinician who will say so plainly, whether that means FormBlends, HealthRX,.com or the manufacturer’s own pharmacy channel for the branded product itself.
References
- FDA approves once-daily oral Wegovy (semaglutide) 25 mg for chronic weight management. Novo Nordisk (company announcement), December 22, 2025. Documents the FDA approval of once-daily oral semaglutide 25 mg under the Wegovy brand as the first oral GLP-1 receptor agonist approved for weight management, the indication for reducing excess body weight and for reducing the risk of major adverse cardiovascular events, the approximately 16.6% mean weight loss with adherence and the roughly one-in-three rate of 20% or greater weight loss cited from OASIS 4, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the planned early-January 2026 US launch.
- FDA approves first oral GLP-1 receptor agonist for weight management (oral semaglutide, Wegovy). U.S. Food and Drug Administration, December 2025. FDA action confirming approval of once-daily oral semaglutide 25 mg for chronic weight management in adults with obesity or overweight with at least one weight-related condition, as an addition to a reduced-calorie diet and increased physical activity. https://www.fda.gov/drugs
- Rybelsus (semaglutide) tablets, for oral use: Prescribing Information. Novo Nordisk / U.S. Food and Drug Administration. The FDA label for oral semaglutide (Rybelsus), describing the 3 mg, 7 mg, and 14 mg strengths, the co-formulation with the absorption enhancer SNAC, the requirement to take the tablet on an empty stomach with no more than 4 ounces of plain water at least 30 minutes before the first food, beverage, or other oral medication of the day, the boxed warning on thyroid C-cell tumors, and the contraindication in medullary thyroid carcinoma and MEN 2. https://www.accessdata.fda.gov/scripts/cder/daf/
- Aroda VR, et al. “Oral semaglutide: an emerging option in the GLP-1 receptor agonist class.” Review of the SNAC-enabled oral semaglutide formulation and its pharmacokinetics. Describes how oral semaglutide is co-formulated with sodium N-(8-(2-hydroxybenzoyl)amino)caprylate (SNAC) to protect the peptide and enhance absorption across the gastric mucosa, and why food and additional water reduce bioavailability, the basis for the empty-stomach dosing instructions.
- FDA approves first oral GLP-1 treatment for type 2 diabetes (Rybelsus). U.S. Food and Drug Administration (news release), September 20, 2019. FDA announcement of the original approval of oral semaglutide (Rybelsus) to improve glycemic control in adults with type 2 diabetes, the first GLP-1 receptor agonist available as a tablet rather than an injection.
- Wharton S, et al. “Oral Semaglutide 25 mg in Adults with Overweight or Obesity (OASIS 4).” N Engl J Med. 2025. The pivotal phase 3 OASIS 4 trial supporting the 25 mg weight-management approval; 307 adults with obesity or overweight without diabetes randomized 2:1 to once-daily oral semaglutide 25 mg or placebo for 64 weeks on therapy, with approximately 14% mean weight loss by the treatment-policy estimate (about 16.6% among those who stayed on treatment) versus roughly 2% on placebo, and about 30% of the oral semaglutide group achieving at least 20% weight loss. Published September 17, 2025.
- McGuire DK, et al. “Oral Semaglutide and Cardiovascular Outcomes in High-Risk Type 2 Diabetes (SOUL).” N Engl J Med. 2025;392:2001-2012. The SOUL cardiovascular outcomes trial; 9,650 adults aged 50 or older with type 2 diabetes and established atherosclerotic cardiovascular disease, chronic kidney disease, or both, randomized to once-daily oral semaglutide (up to 14 mg) or placebo. Over a median 47.5 months, major adverse cardiovascular events occurred in 12.0% versus 13.8% (hazard ratio 0.86; 95% CI 0.77-0.96; P=0.0028), a 14% relative risk reduction. DOI 10.1056/NEJMoa2501006.
- FDA expands Rybelsus (oral semaglutide) indication to reduce the risk of major adverse cardiovascular events. October 2025. Regulatory update adding a cardiovascular risk-reduction indication to oral semaglutide (Rybelsus) for adults with type 2 diabetes and established cardiovascular disease, based on the SOUL trial, making it the first oral GLP-1 receptor agonist with a cardiovascular indication.
- Knop FK, et al. “Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial.” Lancet. 2023;402(10403):705-719. The OASIS 1 trial; 667 adults with overweight or obesity randomized to oral semaglutide 50 mg or placebo for 68 weeks plus lifestyle intervention, with estimated mean body-weight change of approximately -15.1% versus -2.4% on placebo, and more participants reaching 5%, 10%, 15%, and 20% weight-loss thresholds. PMID 37385278.
- Aroda VR, et al. “PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes.” Diabetes Care. 2019;42(9):1724-1732. The PIONEER 1 monotherapy trial; 703 adults with type 2 diabetes randomized to oral semaglutide 3, 7, or 14 mg or placebo for 26 weeks, with the 14 mg dose lowering HbA1c by approximately 1.4% versus 0.3% on placebo and roughly 77% of the 14 mg group reaching HbA1c below 7%. PMID 31186300.